Progressive Multifocal Leukoencphalopathy is a nightmare associated with immunosuppressive treatment of MS and is most common with the migration inhibitors. PML is caused by JC virus with is common and affects most of us. If we are not immunosuppressed we deal with and kill the virus but if your immune system is compromised it is a risk factor. If JC virus gets into the brain it causes death of the oligodendrocyte and therefore it amplifies the damage already seen with multiple sclerosis. Currently JC is not confirmed to be treatable, although there are some things that can help, and may kill a significant number of people (in this study about 10%) and leaves the survivors with disability. If that is not all if you get the virus and PML and stop treatment with a migration inhibitor (natalizumab, fingolimod, siponimod, ozanimod, ponesimod) then because the anti-viral immune cells are alive and they are now able to go in the brain they go into the brain and destroy virally infected oligodendrocytes and so you get damage and this is known as IRIS. This not a flower you want. It stands for Immune Reconstituion Inflammatory Syndrome. So what are the risks?
Here they looked in Europeans with PML and found that higher disability before PML (2 times more), higher load of JC virus in the brain (2.5 times more) and PML symptoms at onset (4 times more) were associated with worse outcomes but the presence of IRIS the outcomes were 70% less. So getting rid of the virus is beneficial. So we need anti-viral treatments and perhaps vaccines. I know, not a lot of comfort to people on natalizumab Plasma exchange to remove circulating natalizumab increased the risk of IRIS

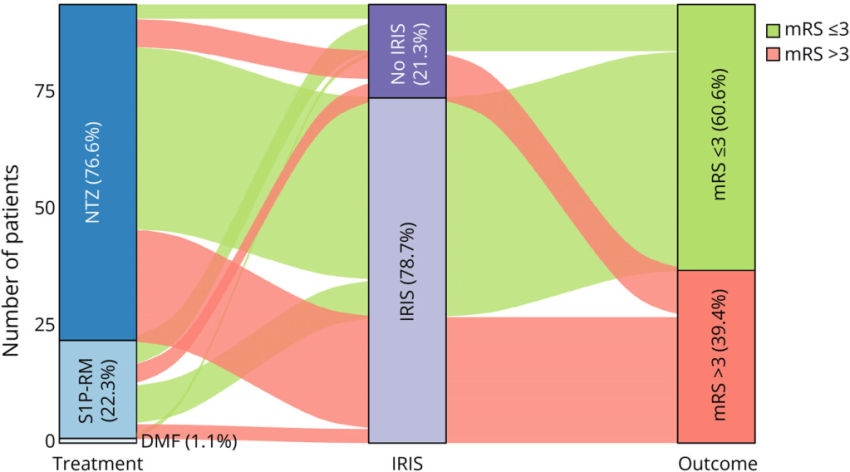
NTZ natlaizumab, S1P-RM fingolimod, siponimod, ozanimod or pnesimdod, mRS modified RankinScale as a marker of disability more than 3 or lower than three (o= no disability) 3 moderate disability requires some help, but able to walk unassisted. 6= death
Blant JC, De Rossi N, Gold R, Maurousset A, Kraemer M, Romero-Pinel L, Misu T, Ouallet JC, Pallix Guyot M, Gerevini S, Bakirtzis C, Piñar Morales R, Vlad B, Karypidis P, Moisset X, Derfuss TJ, Jelcic I, Martin-Blondel G, Ayzenberg I, McGraw C, Laplaud DA, Lebrun-Frenay C, Du Pasquier RA, Bernard-Valnet R; CORPUS and Italian PML study groups. Outcome Predictors in Progressive Multifocal Leukoencephalopathy Associated With Multiple Sclerosis Treatments: A Multicenter Cohort Study. Neurol Neuroimmunol Neuroinflamm. 2026 May;13(3):e200558.
Background and objectives: JC virus (JCV) reactivation causing progressive multifocal leukoencephalopathy (PML) is a complication in patients with multiple sclerosis (MS) treated with disease-modifying therapies (DMTs). Although natalizumab (NTZ) is most frequently involved, PML also occurs less commonly with sphingosine-1-phosphate receptor modulators (S1P-RM), dimethyl fumarate (DMF), and ocrelizumab. This study aimed to identify factors predicting worse outcomes, focusing on the influence of PML-immune reconstitution inflammatory syndrome (PML-IRIS), plasma exchange (PlEx), corticosteroids, and DMT reintroduction.
Methods: This retrospective multicenter cohort study analyzed patients with MS who had JCV-associated pathology (PML or granule cell neuronopathy) from 42 centers (2009-2022). The primary outcome was disability at 12 months, measured by the modified Rankin Scale (mRS). Multivariable analyses identified predictors of poor outcomes, PML-IRIS development, and recurrent MS activity.
Results: Of 96 identified patients, 94 were analyzed. Most cases occurred under NTZ (77%), followed by S1P-RM (22%) and DMF (1%). Twelve-month survival was 91.5%, with a median mRS of 3 [IQR: 2-4]. Multivariable analysis showed that higher pre-PML disability (OR: 1.95 [95% CI 1.46-2.60], p < 0.001), elevated CSF JCV viral load (OR: 2.45 [95% CI 1.55-3.87], p < 0.001), and symptomatic presentation at onset (OR: 3.93 [95% CI 1.23-12.55], p = 0.021) were associated with worse outcomes. Conversely, PML-IRIS was associated with better outcomes (OR: 0.28 [95% CI 0.09-0.86], p = 0.025). PlEx and corticosteroid use had no negative effect.
Discussion: This study provides valuable insights into the management of iatrogenic PML in patients with MS. The findings may guide clinicians in making informed decisions, particularly regarding the use of PlEx, corticosteroids, and the management of PML-IRIS.
Source: multiple-sclerosis-research.org