As you know I get drawn to studies related to things we have been doing and treatment failure due to anti-drug antibodies is on thing they can also result in faster B cell repopulation. But what other things do we know. Well quite a few things like, Age, BMI, Number of Doses, Frequency of Doses e.g. extended dose interval, maybe disease activity prior to treatment is anothere thing one could look at, but the range of repopulation is big with ocrelizumab taking from about 27-275 weeks to get to the lower limit of normal.

So without reading the the paper we get the blah blah blah intro with we did this because its all “unknown/unclear”….loosely meaning our literature review is seemingly not that great because what are looking at has been looked at by others, but we may acknowledge this in the discussion.
Fast forward yep..I was correct and very little reported has not been said before but they raise an interesting point and say “the association between B-cell dynamics and treatment effectiveness, these findings will help guide dosing of anti-CD20 therapies in the future”. But the question is how?
There are questions and one big question is how frequently do we need to dose? Currently companies say every 6 months because they keeps the B cells at a low level. If you were B cell depleting with alemtuzumab or cladribine you would dose for a year and then watch and wait. Why not do the same with ocrelizumab (1 year = 3 dose cycles). We know the answer to this based on the phase II trial data and this shows the interval could be at least 18 months for most, read the literature and it could be at least 30 months for some, but you need to predict the people who will show susbequent disease activity and it is the youth, the people with more active disease pretreatment…but is B cell repopulation a key feature?
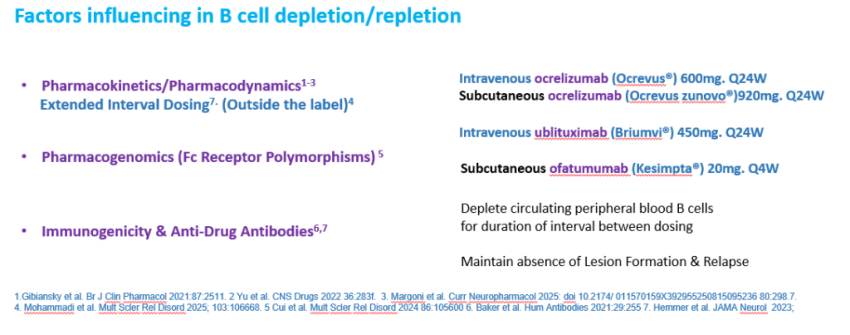
I believe that what comes back is largely not what was there before and what comes back is not the same subset of cells that was there before. The vast majority of recovering cells are naive B cells and the memory B cells remain depleted for months and in many cases years. This the basis of extended interval dosing whereby you stretch out the dosing interval by months, Some people will treated to the time taken for repopulating CD19 B cells to reach a certain level . We know that some people show disease activity with very few or no apparent circulating B cells.

I believe benefit can be had by extending dosing intervals, but it should be tested to ensure it is safe…by extending the interval of dosing you may allow more anti-drug antibodies to appear and this could so the drug working. We apply to do this over a decade ago…no one was interested. However Pharma won’t do these studies as it is not in there apparent interest to sell more drug…..but maybe by doing a formal study they could get a patent on the dosing cycle and keep the bucks to flow in. There are academic trials on extended interval dosing (9-15 months…This isn’t long enough), dosing to repopulating CD19 B cells, or watch and wait.
We could learn from other conditions perhaps as we do not know what is important in terms of the specific B cells cause the problem. Is it the return of EBV infected B cells, or an target specific B cells you could do this more easily in neuromyelitis optica, where relapses are more frequent you could ask when do aquaporin-4 specific B cells return. We could have done this with Prof Angry and he had developed tools to do this. We were doing the background work. We had made contact with Neuros in Brazil and China where there is a lot of NMO and ProfA was hoping to train up some Chinese students, sadly with the passing of ProfA this won’t now happen 
Hogenboom L, McLean A, Schoof L, Taylor L, Strijbis EM, Killestein J, van Kempen ZLE, Kalincik T, Roos I. Predictors of B-cell repopulation in people with multiple sclerosis treated with ocrelizumab: insights from two large cohorts. J Neurol Neurosurg Psychiatry. 2026:jnnp-2026-338533.
Background: Evidence indicates that B-cell dynamics during ocrelizumab treatment vary among individuals with multiple sclerosis. However, our understanding of B-cell dynamics is incomplete. We aim to characterise temporal profiles of CD19+ B-cell repopulation and identify demographic and clinical predictors of B-cell dynamics.
Methods: This was a retrospective multicentre cohort study including people with multiple sclerosis treated with ocrelizumab for ≥180 days from two academic centres. Variables of interest were visualised to explore their associations with CD19+ B-cell count. Generalised linear mixed effect models and logistic mixed effect models were used to identify predictors of CD19+ B-cell counts and early B-cell repopulation (>0.01×109 cells/L, 150-210 days post infusion). We have explored the patterns of early B-cell repopulation and relapse incidence within these groups.
Results: 567 participants, contributing 4592 CD19+ B-cell counts, were included. Younger age (β=-0.01, 95% CI -0.02 to -0.003) (Known from previous numerous studies) , heavier weight (β=0.02, 95% CI 0.008 to 0.02) (Known from numerous previous studies) , fewer ocrelizumab infusions (β=-0.07, 95% CI -0.08 to -0.06) (Known from numerous previous studies)and higher pre-ocrelizumab CD19+ B-cell counts (β=1.42, 95% CI 0.82 to 2.03) were associated with higher CD19+ B-cells during treatment. Pre-ocrelizumab CD19+ B-cells were higher in patients previously treated with natalizumab (mean B-cell count 0.57×109 cells/L (IQR=0.34-0.85)(Known from numerous previous studies) and lower in patients previously receiving sphingosine-1-phosphate receptor modulators (mean B-cell count 0.03×109 cells/L (IQR=0.02-0.13)) (Known from numerous previous studies its a mechanism associated with action) . Early B-cell repopulation was more likely in patients with prior early repopulation (OR=3.00, 95% CI 1.61 to 5.61). Relapse incidence did not differ between the four patterns of B-cell repopulation dynamics (Known from numerous previous studies)
Conclusions: Age, weight, cumulative ocrelizumab exposure, pre-ocrelizumab CD19+ B-cell count and prior disease modifying therapy influence CD19+ B-cell repopulation during ocrelizumab treatment. With further elucidation of the association between B-cell dynamics and treatment effectiveness, these findings will help guide dosing of anti-CD20 therapies in the future.
Source: multiple-sclerosis-research.org