Schoof LG, Hogenboom L, van Kempen ZL, Killestein J, van Oosten BW, Strijbis EM. Reinitiating ocrelizumab with a full 600 mg dose after extended treatment interruption: No increased risk of infusion-related reactions. Mult Scler J Exp Transl Clin. 2026 May 15;12(2):20552173261449688.
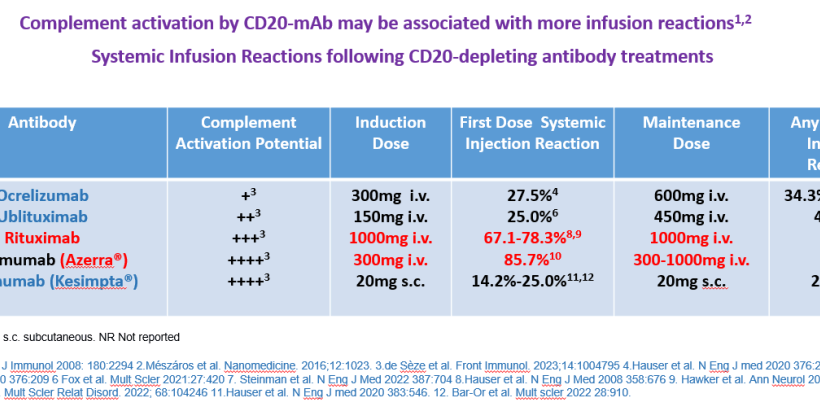
You can get infusion reactions with any depleting monoclonal antibody used in MS, because it is killing the lymphocytes and they are releasing their contents, such as cytokines. This is well known now after the experience with alemtuzumab where it also reactied older lesions and so now it is common to get an dose of anti-histamine, steroids and a paracetamol.

With ocrelizumab (300mg) and ublituximab (150mg) you start treatment with a lower dose than the maintainence (600mg/450mg infusion) dose given every 6 months because on the first dose you are killing all or most of the B cells and they are liberating their contents all over the body and this causes infusion reactions. We know with rituximab and ublituximab that many of the B cells are gone within the first day of treatment, with ocrelizumab I suspect this also the case but the first bit of data is reported at 2 weeks. Ofatumumab gets into the blood slower and at a low dose and perhaps is not as depleting as it takes about 2-4 weeks for B cells to get to their lowest levels in the blood.Ofatumumab has been used in cancer at a much higher dose than used in MS where there were more infusion reactions noted.
After the first cycle of treatment with ocrelizumab or ublituximab there are few B cells to target before the next dose so the infusion reactions are low. We know B cells come back with time and takes about 70 weeks on average with ocrelizumab and ublituximab although there is a big range from about 27 weeks to 275 weeks to get back to the lower limit of normal
This study looks at extended interval dosing of ocrelizumab and suggests that you do not need to start at the 300mg doses two weeks apart. This was found in the normal interval (6 months) or moderate interval (6-9 months) or even the long interval (>9months).
Based on the phase II study you can see it takes time to come back

We already have information on 600mg dosing
Abbasi Kasbi N, Ghadiri F, Sahraian MA, Nahayati MA, Moghadasi AN, Langroodi HG, Poursadeghfard M, Hosseini S, Heidari H, Baghbanian SM, Kamali H, Ameli Z, Shahmohammadi S, Navardi S. Comparing infusion-related reactions of the first full dose (600 mg) biosimilar ocrelizumab administration with the standard divided protocol in multiple sclerosis patients: a randomized controlled trial study. Acta Neurol Belg. 2024;124:205-212.
Background: Ocrelizumab is a humanized antiCD20, thought to be a highly effective disease-modifying therapy (DMT). Its most frequent adverse effects are infusion-related reactions (IRRs). To reduce these reactions, the first dose of ocrelizumab is administered as two 300 mg infusions separated by two weeks. However, in the phase II trial of ocrelizumab, severe IRRs were not significantly different between two doses of 600 mg dose (two separate 300 mg doses) and 2000 mg dose (two separate 1000 mg doses). We compared the IRRs in undivided full (one 600 mg) and divided (two 300 mg) doses of ocrelizumab biosimila
Results: 150 received two 300 mg doses, and 182 received one 600 mg dose of the biosimil. Temporary drug discontinuation was significantly higher in the one 600 mg dose group (p-value < 0.001). However, in the first 24 h, there was no significant difference between two different treatment protocols (one 600 mg dose or two 300 mg doses) in the onset of IRRS (p-value: 0.12).
Conclusion: These findings suggest one 600 mg dose of ocrelizumab administration for the first dose is relatively safe. With some protocol modifications, it could lead to fewer patient referrals, saving time and cost and improvement the access for patients.
This is interesting data because it suggests that you probably will not need to start on low doses if you are switched from one CD20 to another at least from ocrelizumab.
Schoof LG, Hogenboom L, van Kempen ZL, Killestein J, van Oosten BW, Strijbis EM. Reinitiating ocrelizumab with a full 600 mg dose after extended treatment interruption: No increased risk of infusion-related reactions. Mult Scler J Exp Transl Clin. 2026 May 15;12(2):20552173261449688.
Background: Infusion-related reactions (IRRs) are a common side-effect of ocrelizumab (OCR), with the highest risk occurring during treatment initiation. To minimize IRR risk, the first dose is split into two 300 mg infusions over two weeks. Subsequent doses are administered every six months as a 600 mg infusion. After treatment interruptions, some physicians restart with two separate 300 mg infusions due to concern about IRRs. This study evaluates IRR occurrence following a 600 mg infusion after extended treatment interruption. However it has to be said that in primary progressive MS people just got the 600mg
Methods: This retrospective cohort study included all multiple sclerosis (MS) patients who received at least one 600 mg OCR infusion between June 2018 and January 2024 at Amsterdam UMC. Infusions were categorized by interval duration: normal (6 months), moderate (7-9 months) and long (>9 months).
Results: 1438 infusions, in 275 patients, were analyzed. Neither the moderate interval group (306 infusions, OR = 0.914, p = 0.77) nor the long interval group (56 infusions, OR = 0.928, p = 0.575) had significantly higher odds of developing IRRs compared to the normal interval group.
Conclusion: Despite the retrospective design and smaller sample sizes in the moderate and long interval groups, our findings indicate that administering OCR as a single 600 mg infusion after a prolonged interval is safe regarding IRR occurrence.
COI: Yep Multiple
Disclaimer. My views and my data alone
Source: multiple-sclerosis-research.org