This study uses high end technology to delve into the “unclear” and the conclusion is that cladribine gives long-term depletion of memory B cells and then we can say “Should have gone to spec savers” to read our papers from about a decade go. Then they say that naive B cells recover in the CSF and that T regulatory cells appear…So the implications are that this controls the MS and then I think yawn. Is this what the great and the good want to spin. It was a single site paper but had a lot of authors from other sites. They look at what the things the cells in the blood and the brain are producing and then then make their story up. So if you start with 100,000 cells and assay 10,000 cells and there are 9,000 naive cells and 1,000 regulatory cells so they are about 1% of the population and a year later because of the depletion you have only 20,000 cells and you assay 10,000 cells and you have 9,000 naive cells and 1,000 regulatory cells because 90,000 memory cells are depleted the naive B cells increase and the regulatory cells have increased yet they havent changed at all. Yet a story is spun because you want T regulatory cells to increase and explain the mechanism of the drug because that is what dogma says. Now this view above is an extreme comment and may not have anything to do with the explanation and the reality of what was done here, but you have think about these things.
We have shown that when you deplete B cells the memory cells stay low and the recovering cells are transitional/immature and naive B cells as they come from the bone marrow and lymph gland tissue. This response is stereotyped and happens with other B cell depleting agents. Then they shift gear to the T cells which we know have a slow and substained depletion and it is implied that T regulatory cells control everything.
It would have been nice to get a vey detailed look at the B cells rather than a cursory look at everything because you then start to focus on things that may be less relevant to what is the important mechanism of action. This is the beauty of the approach… to keep things complicated so you just keep going. But you get there very slowly. We learn more about the cells in the brain and find there is parallel depletion of some subsets in the blood and the brain, but if one is a feeder to the other this is not surprising. They look for expansions of antigen receptors that could tell us what they are causally reacting to in MS. It could also show that the immune system controls common infections very well. Maybe the latter, as they don’t find much difference in clonality after cladribine. Maybe what comes back after depletion are the cells that protect us from infection and this is one reason why repopulation of immune cells after depletion is not a signal for disease return. So as I said many times before, what comes back is not the same as that present before depletion… So probably depletion is central to the mechanism of action of drugs but what comes back, seldomly correlates with disease control. This is because you are looking at needles in haystacks. This type of study would be best suited to a condition where you know the immune target so you only look at the cells that you know the target something of disease relevance, like aquaporin 4 in Neuromyelitis optica. Doing a simpler condition before doing it in a more complex condition like MS, where you don’t know the targets, may help in determining how you analyse the data. They looked for reactivity against viruses like EBV and found them concentrated in the CNS. I am sure we will see more from the CLOCK-MS study; it has helped me to get handles on what could be going on. But I wonder how much more we will see on cladribine. Will the original manufacturers lose interest as the patent expires and generics arrive?
Smirnov RA, Cantoni C, Lee K, Agnihotri RA, Axtell RC, Salter A, Lancia S, Paley MA, Hayward B, Korich J, Evans E, Pardo G, Obeidat AZ, Stuve O, Bar-Or A, Artyomov MN, Cross AH, Edelson BT, Wu GF. Neurol Neuroimmunol Neuroinflamm. 2026;13:e200565.
Background and objectives: Oral cladribine tablet (CladT) therapy is efficacious for relapsing multiple sclerosis (MS). However, the mechanisms by which cladribine exerts benefit in MS remain unclear, particularly regarding its effects on compartmentalized inflammation within the CSF.
Methods: Transcriptional profiles along with T and B lymphocyte receptor repertoires from CSF and blood were obtained by single-cell sequencing methods from a single site participating in a phase IV clinical trial investigating the impact of cladribine treatment for MS. Blood and CSF samples from patients were obtained immediately before starting CladT therapy, and they were randomized to also provide additional samples at either 5 weeks, 10 weeks, 1 year, or 2 years after CladT therapy. Thirty-four samples from 13 individuals with relapsing MS before and after treatment were available to test the hypothesis that CladT alters the composition and phenotype of lymphocytes in the CSF, including paired baseline and post-CladT CSF samples obtained from 4 unique participants.
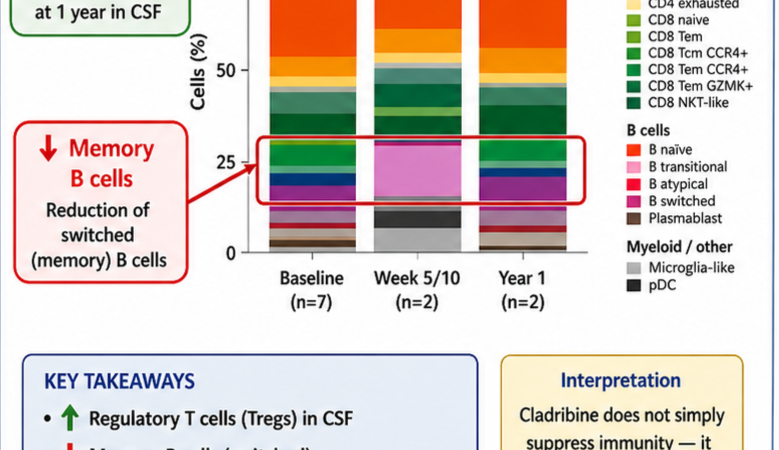
Results: We found that treatment with CladT profoundly altered cellular composition, but not the transcriptional phenotype, of immune cells in the CSF. In particular, we identified a reduction in switched memory B cells but recovery of naive B cells in the CSF, similar to our findings in blood. In addition, populations of CD4 Treg cells emerged early after CladT therapy and remained elevated 1 year later in the CSF, but not in the blood. Antigen receptor sequencing revealed a moderate decrease in numbers of large clonally expanded CD8 T cell clones (>10 cells/clone) primarily in the CSF, but also in the blood after CladT treatment.
Discussion: Our results identified unique cellular dynamics and changes in T cell and B cell clonality in both tissues, which can potentially explain long-term beneficial effects of CladT therapy in MS, including preservation of immune function and a relatively low number of side effects. Altogether, this study demonstrates that CladT treatment had a substantial impact not only on blood but also on the CSF compartment, highlighting the importance of cross-tissue analysis for better understanding of effect and the mechanism of action of disease-modifying therapies.
COI: None
Disclaimer
Source: multiple-sclerosis-research.org