Thanks for the support in relation to my post on friday…this wasn’t a post to say woe is me, it was to inpart explain the inconsistencies in posts and the difficulties in finding time to post. However, yesterday I moved into my new home….OK still have to get the furniture, but I will soon have my own bed.
For many, many years MS was a largely T cell mediated disease and this focused the minds of people of how MS should be dealt with…but the most interesting experiement is the clinical trial as a positive study tells you about disease and a well-performed negative trial tells you something too once you realise that there are plenty of negative trials that are not well performed. The curve ball that occurred was the possitive impact of CD20-depletion on relapsing and active progressive MS…How does that work? CD20 is a relatively B cell specific target.

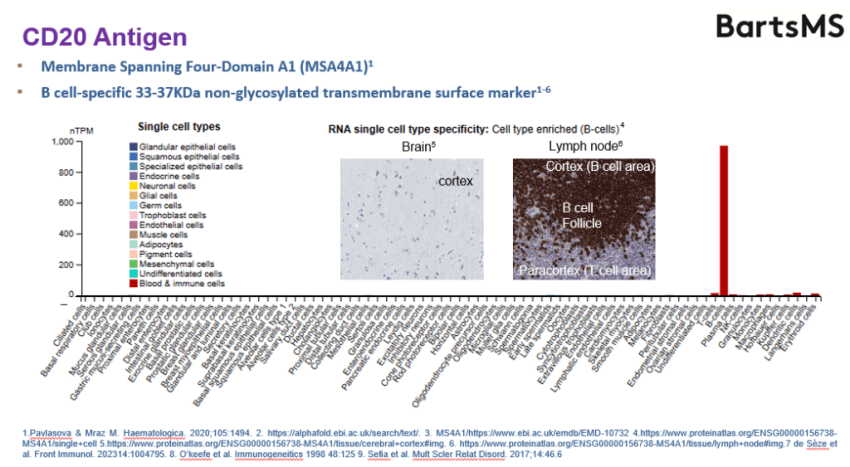
The red anove is CD20 expression in a variety of different cells. You can see it easily on B cells the big bar to the left is T cells…yet some crazy idea has been spread that it works because CD20 is expressed by a subset of CD20 T cells…Yes it has to be considered to be possible but why concoct a hard sell story that has more holes than a bit of Emmental cheese when there is a simple explanation i.e. it is killing B cells.
All CD20 B cell depleters reported in MS work. CD20 binds to a subset of B cells not the very early B cells and not the antibody secreting cells.
However simply targeting B cells is not a recipe for success. Blocking CD267 or TACI or the BAFF receptor at best did not work and even it is suggested made MS worse. Targeting Brutons Tyrosine Kinase with tolebrutinib did not inhibit relapsing disease compared to teriflunomide and perhaps was worse. In the two phase III trials there was more MRI lesions nearly double in the tolebeutinib groups but they didn’t bother to do the stats because it didn’t inhibit the relapse rate. Best not draw more attention to a bad result.

CD19 is another B cell specific marker that really insn’t on T cells yet targeting of CD19 also inhibits MS as shown by CD19-antibody mediated depleting antibody and also by CD19 CAR-T therapy. To me this says stick the CD20 T cell idea in your pipe and smoke it. (meaning). The CD20 T cell targeting idea is unlikely to be the true explanation, yet I have seen it defended and the great and the good play their part in this.
Anyway, antibody is 99.9% excluded from the CNS whereas CAR-T cell therapy can get into the brain…But as the antibody works it sort of says, much of the action created by B cell depletion occurs outside of the brain. If a B cell doesnt get survival signals it will die and we know that if you deplete B cells in the blood, the inflammation in the brain including T and B cell inflammation dies. So turn off the tap and the water disappears down the unplugged plug hole.

CD19 CAR-T therapy is where you make T cells target CD19 and so they kill B cells and this was designed for destruction of B cell cancers. As these can cause rapid lethality in people the benefits outweigh the risks, but destroying B cells forever could have consequences. However it seems that this theorhectical issue is not the reality and the CAR-T cells disappear in most people and B cells return. CD-19 CAR=T therapy works in MS as there are small academic trials that have already shown this.
However after telling us that MS is caused by B cells, some bods now tell us that MS is an antibody mediated disease. Now I am not sure this is quite right because therapies that can remove antibody secreting cells have not blocked relapsing MS. However there are CAR-T cell therapies that will target antibody secreting cells because they express BCMA
B-cell maturation antigen (BCMA), also known as tumor necrosis factor receptor superfamily member 17 (TNFRSF17), which recognizes B -cell activating factor (BAFF) it called CD269. It expressed by antibody secreting Plasmablasts and plasma cells. So CAR-T therapy against BCMA has been tried in MS.
Neuromyelitis optica responds to BCMA CAR-T cells and responds to CD19-depleting antibody therapy and that is good because we believe that antibodies against aquaporin 4 cause the problems. However neuromyelitis optica also responds to CD20 depletion and CD20 is not on antibody cells so how does it work? So I have always wondered what will happen in MS and now we get some insight. I have said that the Chinese docs have really got CAR-T cell therapy going and now we see what happens. They have targeted progressive MS, where it has been argued by people including me that antibodies could have some role in the pathology.
The failure of anti-BAFF and APRIL which bind to the BCMA moleule to give naive B cells and notably plasma cells a survival signal points the finger away from these cells as being central drivers of MS and the success of anti CD20 thereofre points to memory B cells are being important as they largely do not express BCMA, so it could predict that targeting plasma cells with anti-CD38 or anti-BCMA may not work in MS. However progressive MS has been suggested to have a component where antibody with drive pathology by the microglial cells. So I am super interested to read the new paper surfacing

Qin C, Dong MH, Zhou LQ, Chu YH, Pang XW, He JY, Shang K, Xiao J, Zhu L, Ye H, Cai SB, Wang D, Bu BT, Meyer Zu Hörste G, Li CR, Tian DS, Wang W. Anti-BCMA CAR-T therapy in patients with progressive multiple sclerosis. Cell. 2025:S0092-8674(25)01088-8.
Progressive multiple sclerosis (PMS), which is characterized by relentless disease progression, lacks effective treatment. While recent studies have highlighted the importance of B cells in driving compartmentalized central nervous system (CNS) inflammation in PMS pathogenesis, current B cell depletion therapies, such as CD20 monoclonal antibodies, face challenges in targeting plasma cells within the CNS. Here, we treated five patients with PMS (one primary PMS and four secondary PMS) with anti-B cell maturation antigen (BCMA) chimeric antigen receptor T (CAR-T) cell therapy in an ongoing phase 1 clinical trial (ClinicalTrials.gov: NCT04561557). Only grade 1 cytokine release syndrome was observed, and all grade ≥3 cytopenias occurred within 40 days post-infusion in all five patients. Meanwhile, we detected plasma cell depletion in CNS compartments, prolonged expansion and relieved exhaustion of CAR-T cells in the cerebrospinal fluid, and attenuation of microglial activation. These findings provided insights into the potential application of anti-BCMA CAR-T therapy for advancing clinical management of PMS.
So Highlights
•Five progressive multiple sclerosis patients were treated with anti-BCMA CAR-T therapy
•The treatment caused plasma cell depletion in the central nervous system of the patients
•The CAR-T cells showed prolonged expansion and reduced exhaustion in cerebrospinal fluid
•The treatment alleviated microglial activation in cerebrospinal fluid
So far so good its what the biology suggests could occur however reductions in cell numbers and free kappa light chainss can be the product of peripheral B cell depletion and the consequence of this over time and it has to be said that 3 of the 5 had been treated with anti-CD20 and as this study has not been controled. Furthermore all of the people were given a lymphodepleting chemotherapy regimen comprising fludarabine and cyclophosphamide daily (These enter the brain and will kill dividing cells in the blood and the brain and will target B cells) and also fludarabine another immune depleting which kills non-dividing cells and so sadly it is fatally flawed experiment to answer my question as this chemotherapy will destroy the memory B cells in the periphery and this will I am sure inhibit relapsing MS. This is the problem of intrepreting HSCT and CAR-T therapy as the conditioning therapy used to create space in the blood for the transfer of cells will inhibit MS irrespective of whether they get the HSCT or CAR-T therapy….so sadly without proper control, linking cause and effect is difficult. It was evident that there was T and B cell depletion They say “All five patients demonstrated improvement in EDSS scores, accompanied by significant reductions in both Nine-Hole Peg Test and Timed 25-Foot Walk duration, along with the decrease in CSF neurofilament light-chain (NfL) level (4/5)” N radiological disease activity was observed, with no new T1 gadolinium-enhancing lesions or new/enlarging T2 lesions in any patient at any time point after CAR-T cell therapy. Moreover, a reduction in T2 lesion volume was noted in two cases”
There were drops of T and B cells in blood bone marrow and blood and there were loads of CSF samples taken..There was sustained reduction in free light-chain levels, partial resolution of OCBs,…This was abit diappointing as I was hoping for eradication of oligoclonal bands however the data isnt shown in a clear way. Antibodies will hang round for some time after depletion of the cells. You can reduce free-light chains and notably partially reduce OCB with cladribine, anti-CD20 antibody, CD19-CAR-T and HSCT.
However, the question that was not addressed is what is the impact of this type of therapy on antibody responses to vaccines and past infections. I guess with some reading this can be found out as anti-BCMA licenced therapy and this question must have been addressed, maybe something that Luis can hunt down. There are many questions still to be answered, but this paper was abit of light in the dross that I have been posting in on.
COI: None
Source: multiple-sclerosis-research.org