Thomas et al. Anoctamin-2-specific T cells link Epstein-Barr
virus to multiple sclerosis. Cell (2026), https://
doi.org/10.1016/j.cell.2025.12.032
Epstein-Barr virus (EBV) infection constitutes a prerequisite for multiple sclerosis (MS) development, and cross-reactivity between EBV nuclear antigen 1 (EBNA1) and anoctamin-2 (ANO2) antibodies was previously demonstrated in persons with MS (pwMS). Here, we show that ANO2-specific CD4+ T cells are more frequent in pwMS. Immunization of SJL/J mice with ANO2 or EBNA1 led to cross-reactive CD4+ T cell and antibody responses. ANO2 pre-immunization led to exacerbated experimental autoimmune encephalomyelitis (EAE), an effect mediated by CD4+ T cells, as confirmed by adoptive transfer experiments. T cell clones with cross-reactivity to EBNA1 and ANO2 could be isolated from natalizumab-treated pwMS, and sequencing of EBNA1- and ANO2-specific T cell receptors (TCRs) revealed a significant repertoire overlap.We thus report the first mechanistic evidence that EBNA1 CD4+ T cells can target the MS autoantigen ANO2, thereby establishing a link between EBV infection and neuroinflammation.
What causes MS?
The view has been made that immmune responses to EBNA1 of Epstein bar virus cross react to proteins in the MS. About 2-3 years ago when the MS-World eventually went EBV mad, there was little discussion on what happened to the years of work telling us that MS was a T cell -mediated disease to myelin basic protein and why there was a sudden change of direction and we were told to be convinced that what causes MS was an antibody response to a small part of EBV that cross reacted with the bit of a target called GlialCam that was inside the astrocyte or to a lesser extent oligodendrocytes and liver cells.
It didn’t occur in every body leaving other candidate possibilities and sure enough we have had a few other suggested such as alpha B crystallin and Anoctamin-2 to mention a few. Now I would say that not everybody can repeat the original or subsequent findings. But this process of cross reactivity is called molecular mimicry, which was originally based on an idea based on observations of T cell target binding.
I can buy the idea that Epstein Barr Virus is the cuprit in the causal pathway and I can also buy tthe idea that there is some cross reactivity of immune reponses to EBV can cross react with CNS target. You can shown it, but it is it causal?
ProfG is not so sure of its importance and asked me what problems do I see with the idea? Now what every I say, it is an opinion and could be wrong and you would want a counter view. If you look hard enough to show this, I am sure you can find it. But it does not say it is causal but could be an effect of the cause. You also have to ask what other targets do EBV targeting antibodies bind, to as we have recently had a link between EBV and Lupus and other conditions.
So cross reactivity can be shown but if all you do it prove the idea and do nothing to disprove the idea (easier) you simply do what you want to give you the answer you want.
So the Ugly Sisters want to marry the Prince and so they squeeze their feet in to the dainty shoes of Cinderella and claim their prize. But if you measure the shoe and get the proper size of foot that would fit the shoe and then measure the ugly sisters shoe and find they are abit big, or too small for that matter, you start to get the idea that the ugly, or for that matter beautiful, sister is not the belle of the ball, who left her shoe with Prince Charming. Now I am being flipant her…But in reality these days very little is done to question dogma, to show that the idea is not correct.
Now the post is not really about this paper
These days nobody does any work, so what does ChatGTP say to the question?
Why is anoctamin-two a good autoantigen target for multiple sclerosis (first answer given below)
“Anoctamin-2 (ANO2, also called TMEM16B) has been proposed as a good candidate autoantigen in multiple sclerosis (MS) because it fits several features that make a protein capable of driving CNS-specific autoimmunity. Here are the key reasons, step by step.
1. Strong and selective expression in the CNS
ANO2 is a calcium-activated chloride channel that is:
- Highly expressed in neurons (especially in the cortex, hippocampus, and olfactory bulb)
- Also detected in oligodendrocytes and myelin-associated regions
MS is a central nervous system–restricted autoimmune disease, so proteins with predominant CNS expression are more plausible targets than ubiquitous proteins.
2. Limited peripheral immune tolerance
Proteins that are:
- Low or absent in the thymus
- Poorly expressed in peripheral tissues
are less likely to induce central immune tolerance. Evidence suggests ANO2 expression outside the CNS is minimal, meaning:
- Autoreactive T or B cells specific for ANO2 may escape deletion
- These cells can later become pathogenic when exposed to CNS antigen
This is a classic feature of many MS-relevant autoantigens.
3. Accessibility during inflammation and neurodegeneration
Although ANO2 is normally intracellular or membrane-embedded:
- Blood–brain barrier breakdown
- Neuronal or oligodendrocyte damage
- Inflammation-induced antigen release
can expose ANO2 peptides to antigen-presenting cells. Once exposed, ANO2 can be:
- Processed and presented on major histocompatibility molecules
- Targeted by autoreactive T cells or antibodies
This fits well with MS pathology, where tissue damage and immune activation reinforce each other.
4. Demonstrated immunogenicity in MS patients
Studies have shown that:
- Some MS patients have T-cell responses to ANO2-derived peptides
- Others show autoantibodies recognizing ANO2
Importantly, these responses are:
- More frequent or stronger in MS than in healthy controls
- Often associated with inflammatory disease phases
This distinguishes ANO2 from bystander antigens.
5. Functional relevance to MS symptoms
ANO2 contributes to:
- Neuronal excitability
- Signal modulation and firing patterns
Autoimmune targeting of ANO2 could therefore contribute to:
- Neurodegeneration
- Synaptic dysfunction
- Fatigue, cognitive symptoms, or sensory abnormalities
This makes it not just an immune target, but a pathophysiologically meaningful one.
6. Fits the “multiple autoantigen” model of MS
MS likely does not have a single universal autoantigen. Instead:
- Different patients target different CNS proteins
- Epitope spreading occurs over time
ANO2 fits well as:
- A subset-specific or stage-specific autoantigen
- Part of a broader autoimmune repertoire including myelin and neuronal proteins
In summary
Anoctamin-2 is considered a good MS autoantigen candidate because it:
- Is CNS-restricted
- Escapes strong immune tolerance
- Becomes exposed during CNS inflammation
- Elicits immune responses in MS patients
- Has functional relevance to neuronal pathology
What do you think? Do you buy it?
So now we go the other way and ask
Why is anoctamin-two not a good autoantigen target for multiple sclerosis? (first answer given below)
Although anoctamin-2 (ANO2 / TMEM16B) has been proposed as a candidate autoantigen in multiple sclerosis (MS), there are strong reasons why it is unlikely to be a primary or broadly relevant MS autoantigen. These limitations are important in understanding MS pathogenesis.
1. MS pathology is dominated by myelin damage, not neuronal membrane targets
The hallmark lesions of MS are:
- Demyelination
- Oligodendrocyte loss
- Inflammatory plaques centered on white matter tracts
ANO2 is:
- Predominantly neuronal, not myelin-specific
- Sparse in compact myelin compared with classic targets like MBP, MOG, PLP
If ANO2 were a major autoantigen, one would expect:
- Primary neuronal pathology early in disease
- Widespread channelopathy-driven symptoms
Instead, neuronal injury in MS is usually secondary to demyelination and inflammation.
2. Poor accessibility to the immune system
ANO2 is:
- A transmembrane ion channel
- Mostly located in intracellular membranes or neuronal plasma membranes
For B cells and antibodies especially:
- Conformational extracellular epitopes are limited
- Most ANO2 domains are inaccessible unless cells are destroyed
This makes ANO2 a weak initiator of autoimmune responses compared with surface-exposed myelin proteins (e.g., MOG).
T cells see small linear epitopes where as antibodies and notably the important ones typically see shapes and not linear sequences and the supporting data is only based on linear amino acid structures
3. Immune responses may reflect epitope spreading, not causation
Evidence for ANO2 reactivity in MS patients is:
- Inconsistent
- Found only in subsets of patients
- Often detected in later disease stages
This pattern strongly suggests:
- Secondary immune responses following tissue damage
- ANO2 becomes targeted after inflammation is established, not before
In MS, many non-pathogenic autoantibodies arise as a consequence of CNS destruction.
4. Lack of robust animal model causality
A strong MS autoantigen should:
- Induce experimental autoimmune encephalomyelitis (EAE) reliably
- Reproduce demyelination and paralysis when used as an immunogen
ANO2:
- Does not consistently induce EAE
- Does not reproduce canonical MS-like pathology when targeted alone
In contrast, MOG and PLP robustly trigger EAE across species and strains.
5. Weak genetic and HLA associations
True disease-driving autoantigens often show:
- Strong binding to MS-associated HLA alleles (e.g., HLA-DRB1*15:01)
- Clear genetic risk correlations
ANO2 peptides:
- Show limited or inconsistent HLA restriction
- Lack strong linkage to MS risk alleles
This reduces the likelihood that ANO2 is a central antigen in disease initiation.
6. Poor disease specificity
Autoantibodies to ANO2 have been detected in:
- Other inflammatory neurological conditions
- Some non-inflammatory contexts
This weakens its utility as:
- A diagnostic biomarker
- A disease-defining antigen
MS autoantigens tend to show CNS specificity plus disease enrichment.
7. Targeting ANO2 would be therapeutically risky
From a therapeutic standpoint:
- ANO2 is important for neuronal excitability and signaling
- Immune targeting or tolerance induction could disrupt normal neuronal function
This makes ANO2 a poor therapeutic target, even if autoimmunity exists.
Bottom line
Anoctamin-2 is unlikely to be a primary or universal MS autoantigen because:
- MS is primarily a myelin-directed disease
- ANO2 is poorly accessible and mainly neuronal
- Immune responses to ANO2 are inconsistent and likely secondary
- It lacks strong experimental, genetic, and pathological support
At most, ANO2 may represent:
- A secondary antigen arising from epitope spreading
- A marker of ongoing neurodegeneration rather than a disease driver
So first thing is look answer to Point 1 (Top) and point 1 and 6 (Bottom comment) they do not say the same thing and in fact say the opposite. Do you accept both answers as true of has Chat GTP made it up? What do you believe.
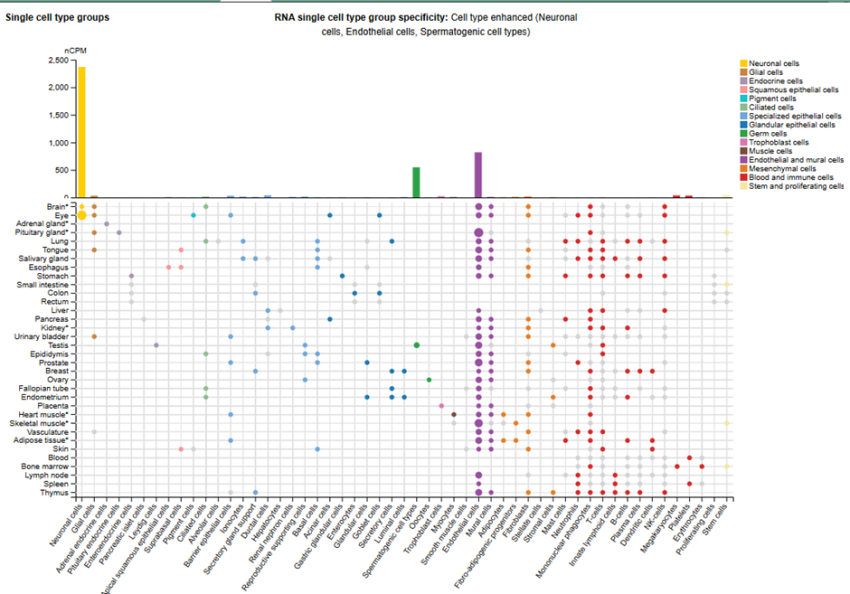
Distribution of Anoctamin-two is available from multiple sites I dug this out from http://www.proteinatlas.org searching for Ano2.

Expression is high in nerves notably the retina in eye and on blood vessels and thes are found all over the body, so why would you get brain disease in ANOC2 was important?
It is found in the nerves that detect light (rods & cones). Why is MS not a blinding disease?

There is weak expression on oligodendrocytes and attack of the blood vessels may be more exprected surely

However this shows responses in MS and then moves to mice, I can’t read the pdf I got and cannot comment, but if you can detect antibody responses to a protein you may expect to be able to detect T cell responses too. Furthermore, if you have nerve damage due to something else you may expect the protein to be released and so is it an effect or a cause?….You can’t work that out just by looking, ideally you block the immune response to the protein and the disease goes away. But it is not a straight forward and easy thing to do.
That you don’t get EAE to a protein is not proof that it is not important, however the target is not really expressed much in the CNS you wouldnt expect it too either. Three mice strains were tested but these are essentially three individuals. In these mice we know some myelin proteins cause disease and dom do not. Some proteins dont cause disease in some strains HLA-DR is more structurally like H-2E in mice but neither C57BL/6 (H-2b), NOD (H-2g7) nor SJL (H-2s) express H-2E because they do not express the H-2E alpha chain, NOD and C57BL/6 mice are rather genetically resistant to EAE and give poor response to MBP, PLP react to MOG to give non relapsing disease. SJL mice respond to MBP, PLP and MOG and can develop relapsing disease but react to different peptide (15-20 amino acid stretch) specificities meaning a small section of MOG induce disease in one strain but not in another. If expression of ANO2 is high in the eye would the mice get eye disease, well not for the SJL as they a geneticaly prone to lose photorecptor nerves as they carry the Rds (retinal degeneration slow peripherin 2 gene). But what they did was inject animals with anoctamin-2 peptides and often didn’t find disease although they got T cell responses and antibody response…When MOG was first found to be a potential autoantigen it too did not cause disease, but it induced antibodies and if you opened the blood brain barrier with MBP specific T cells it allowed antibodies to get in and disease was caused. So here they immunize ANO2 and then reimmunise with PLP in SJL mice you get worse disease….However ProfLove showed that if you persist and break proteins down you can often find disease causing/imune enhancing regions. But as it was shown if you have antibodies reactive to nerve proteins and you open the blood brain barrier you can get augmented disease. Does it prove that ANO2 is the problem in MS?. Well not really, ProfLove looked at alpha B crystallin and didnt get disease in most mice but once she did and it turned out this was the only mouse where alpha B crystallin was expressed in the oligodendrocyte, could we scour the data base to find a microrobe with a sequence that cross reacts with MOG, well there are only 20 different amino acids and within any linear sequence the immune system only has to see a few in the correct location to be activated I suspect you could find cross-reactivity if you looked I once took the EBNA-1 peptide reported to important in MS and search and myelin antigens were not the top hits of similaities and likewise if you search myelin sequences with microrobes you find many candidates such as bacteria that have them.
How was years of T cell work as a primary culprit dismissed to turn that the idea that MS is T cell mediated into an idea that antibody is the important element. Likewise how were many years of work supporting the rubbish idea (just an opinion) of myelin basis protein being the target in MS binned to change it to be against a liver and astrocyte target in glialcam
Source: multiple-sclerosis-research.org