Cladribine enters the CNS and about 25% of the levels in the blood reach the brain and so active levels of cladribine can enter the CNS. In this study they say “Regarding OCBs status, OCBs disappeared in five patients while they were detected in two patients (A total of 39 gave repeat samples) who previously turned out negative and 32 were positive, so about 32/37 remained positive (86%). This sounds familiar
Marastoni D, Eccher C, Signori A, Anni D, Foschi M, Crescenzo F, Mazziotti V, Virla F, Sicchieri M, Turano E, Tamanti A, Camera V, Ziccardi S, Zanetti G, Pizzini FB, Martini S, Fratucello A, Bonetti B, Sormani MP, Calabrese M. The effect of cladribine tablets on intrathecal inflammation in relapsing-remitting multiple sclerosis. J Neuroinflammation. 2026 . doi: 10.1186/s12974-026-03725-2.
Background: To investigate the intrathecal effect of cladribine tablets on cerebrospinal fluid (CSF) inflammatory proteomic profile, cortical lesions (CLs), paramagnetic rim lesions (PRLs) number and cognition after 2 years of treatment.
Results: Forty-two patients with RRMS treated with cladribine tablets were enrolled in a prospective longitudinal 2-year study. All patients were scheduled to undergo a lumbar puncture before treatment initiation and after 2 years of treatment, a clinical evaluation, including Expanded Disability Status Scale (EDSS) assessment, every 6 months, and a 3T MRI every year. White matter lesion number and volume, CLs, PRLs number and neuropsychological status were evaluated. CSF levels of 17 inflammatory markers were assessed by multiplex immune assay. No evidence of disease activity (NEDA) was defined as the absence of relapses, MRI activity and 6-months confirmed disability progression, defined as an increase of ≥ 1 point in the EDSS. Thirty-nine patients completed the study, and 33 agreed to repeat the lumbar puncture. After two years, 23 (59%) patients retained the NEDA status. Cladribine tablets reduced most of the inflammatory markers in the CSF of patients, with a significant reduction, after correction for multiple comparisons, in levels of sTNFR1, Pentraxin3 and CCL22. No patients accumulated new CLs, and no significant changes in PRLs and cognition were observed over the follow-up.
Conclusions:Cladribine tablets administration led to a reduction of intrathecal inflammatory markers. These findings, along with the absence of CLs and PRLs accumulation, suggest a potential effect of the drug on intrathecal compartmentalized inflammation.
There is interest in targeting inflammation into the CNS
Correale J, Halfon MJ, Jack D, Rubstein A, Villa A. Acting centrally or peripherally: A renewed interest in the central nervous system penetration of disease-modifying drugs in multiple sclerosis. Mult Scler Relat Disord. 2021;56:103264. doi: 10.1016/j.msard.2021.103264.
Notably cladribine enters the CNS at active levels and so the idea that it may inhibit inflammation in the CNS, So did it inhibit oligoclonal bands in the CNS. This idea prompted profK to look in the CNS.
He thought he would do it after subcutaneous cladribine…
- Allen-Philbey K, Stephenson S, Doody G, MacDougall A, Aboulwafaali M, Ammoscato F, Andrews M, Gnanapavan S, Giovannoni G, Grigoriadou S, Hickey A, Holden DW, Lock H, Papachatzaki M, Redha I, Baker D, Tooze R, Schmierer K. Effects of cladribine on intrathecal and peripheral B and plasma cells. Clin Exp Immunol. 2025;219:uxae116. doi: 10.1093/cei/uxae116
but thought then why not do it it with oral cladribine
2. Ammoscato F, Wafa M, Skonieczna J, Bestwick J, Monero R, Andrews M, De Trane S, Holden D, Adams A, Bianchi L, Turner B, Marta M, Schmierer K, Baker D, Giovannoni G, Gnanapavan S. Cladribine tablets in relapsing-remitting multiple sclerosis preferentially target B-cells. Clin Immunol. 2024 Dec;269:110380. doi: 10.1016/j.clim.2024.110380.
Then Merck thought they would do it also
3. Schmierer K, Wiendl H, Barkhof F, Montalban X, Achiron A, Derfuss T, Chan A, Hodgkinson S, Prat A, Leocani L, Sellebjerg F, Vermersch P, Jin H, Sponton L, Chudecka A, Gardner L, De Stefano N. Clinical and mechanistic effects of cladribine in relapsing multiple sclerosis: 2-year results from the MAGNIFY-MS Study. Ther Adv Neurol Disord. 2025 Jul 31;18:17562864251351760.
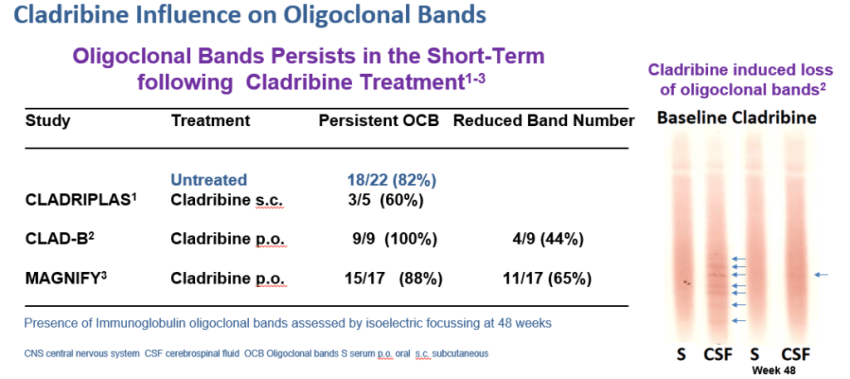
Guess what? The results were remarkably consistent and sadly there were persistent oligoclonal bands

references: Above.
So they all say the same thing. i.e. although the number of oligoclonal band deceases, they persist for some time, but may disappear. The makers of oral cladribine suggest this is evidence that cladribine works in the CNS…but we need to be aware that plasma cells that make antibodies do not really express the target for cladribine, so it is not going to get rid of oligoclonal bands because long-lived plasma cells are going to be relatively cladribine insensitive. Anti-CD20 (ocrelizumab target) or anti-CD52 (alemtuzumab target). Now CD19-CAR-T does the same so more clamour for an effect in CNS, but in addition ocrelizumab does the same as cladribine and it will be CNS-excluded by 99.9% and importantly natalizumab does the same and remember it will be CNS excluded but important the action of importance is outside of the CNS.
If one does a study and looks 2 years later and conclude because there inflammation is reduced in the CNS, it says cladribine is active in the CNS…Isn’t this about of a NSS moment. Now imagine that we use an agent that doesn’t get into the CNS like most MS drugs, but blocks the cause of inflammatory lesions from entering the CNS and so MRI lesions don’t occur and as such there won’t be immune cells in the CNS…so what is the difference with the study looking at cladribine here. Because cladribine inhibits lesions there will be less inflammation in the CNS. This was presented by the group at ECTRIMS 2024.

Mario Picozza, Damiano Marastoni, Chiara Eccher, Alice Verdiani, Daniela Anni, Andrea Misiti, Federica Virla, Ermanna Turano, Valentina Camera, Giovanna Borsellino, Luca Battistini, Massimiliano Calabrese,
Many years ago it was shown that if you look at cells in the CNS months after treatment with anti-CD20 there were fewer T cells and B cells in the CNS, and this was viewed as evidence that CD20 works because it depletes T cells. Emmmm surely disease control simply means less cells in the CNS. It’s not rocket science.
So at the same 2024 meeting we had another group doing the same thing but in this case they didn’t wait for 2 years to look but 5 weeks.

This is interesting as by looking at MRI studies it is evident that cladribine has activity within 5-10 weeks so it is consistent with the importance of depletion of cells within the memory B cell subset.
Get rid of B cells from the blood and they are gone from the blood and brain within 5-10 weeks you don’t have to wait for 2 years. Now a B cell without survival factors will rapidly die but if they get them they can differentiate towards cells that can secrete antibody. Importantly the loss of memory cells will mean that plasmablasts and short-lived plasma cells will not be produced (as cell type that can come from differentiation cell of B cells) in the CNS and oligoclonal bands will drop.

Cladribine will deplete short-lived plasma cells (antibody secreting cells)
The number of bands will drop

With time some of the long-lived antibody secreting plasma cells will die and some people may become oligoclonal band negative with time.

The loss of oligoclonal bands is a common mechanism with many MS drugs suggesting that by targeting B cells in the blood you can reduce the influence of short-lived antibody secreting cells in the CNS. So there may be nothing that special with cladribine as agents that may not act in CNS may do something similar. However this effect could be more active or quicker for agents that get into and act the CNS.

This is just an idea and could be wrong, but it explains the observations. But it is important to be aware of cause and effect. Is the effect being observed simply a down stream consequence of something else upstream that is more important and worth getting rid off.
COI Multiple
Disclaimer: My views
Source: multiple-sclerosis-research.org