The idea for CD20 immunotherapy is…. deplete the B cells in the circulation and they cannot get into the CNS. If they do not get into the CNS there will be no/few lesions and no/few relapses. There are lots of different anti-CD20 antibodies and when you select the dose you aim to deplete the B cells in the blood for a month with ofatumumab and 6 months with rituximab, ocrelizumab, and ublituximab.
Making the exact numbers up if you need 20mg to deplete B cells for at least a month and the half -life for half of the antibody to disappear is a month it means for a 6 monthly dose you need to inject 800mg. Basically if you inject 800mg after one month 400mg is around 2 months 200mg is around after 3 months 100mg is around after 4 months 50mg is around and after 5 months 25mg is around and still working. Get another antibody that needs 10mg to do the depletion you simply start off with 400mg.
So the way you do it, you give the dose to achieve the same biology.
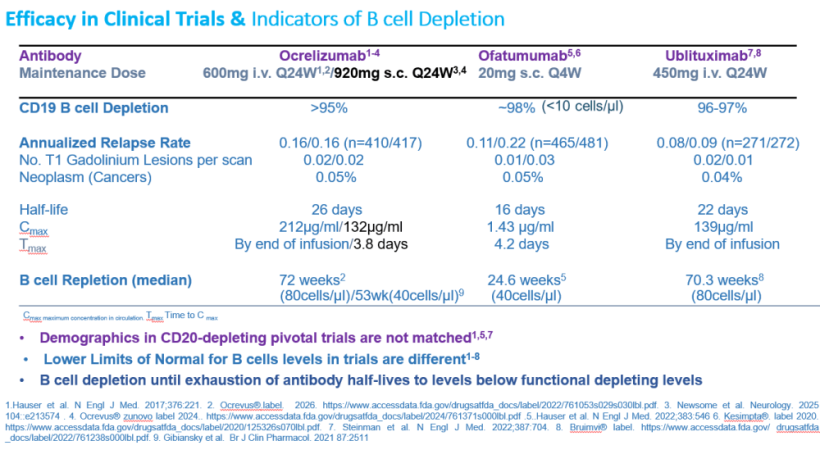
For ocrelizumab you give 600mg, for ublituximab it takes 450mg and for rituximab they give 500-1000mg. So if removing B cells from the blood is the mechanism wanted and you select doses to do this, then there is a a biological similarity . Then why would you expect there to be a difference between the agents? In this study from Finland (belwo) they find that ocrelizumab and rituximab behave in a similar way and exhibit comparable efficacy.
Although the people in the trials are different and you need to be cautious in doing comparisons, I would say the three approved B cell depleting antibodies deplete B cells in the blood and all inhibit relapsing disease with high efficacy.

Now if I shift the goal posts and say to inhibit progression independent of any effect on relapse you need to get the antibody into the brain. One wonders if they would be the same.
If we look at rituximab we know what happens when you give antibody in the blood, and into the CNS in the brain or spinal cord and we know the depletion in the blood, in the lymph glands, spleen and bone marrow. We can see that following rituximab 99.9% of the antibody never reaches the CNS and when it does the B cell depleting mechanisms, requiring complement (initiated with C1q) mediated killingand/or natural killler cells that mediate antibody dependent cell killing, are relatively lacking.

But if you look at the maxium concentration of the drug in the blood following ofatumumab is about 100 times less than with ocrelizumab and ublituximab now a thousand of what is in the blood gets into the CNS that means perhaps that ony 10ng/ml reaches the CNS for some antibodies, I am not sure that is enough to do alot. But then I do not think it really matters as I think the action of the CD20 antibodies is in the blood. If the B cells don’t get in CNS then they don’t support the cells that are in the CNS and of a B cell if you do not get survival signals the B cells die. We know that with rituximab that if you give treatment and then look in the CNS 6 months later the B cells are largely gone as well as many T cells even though anti-CD20 is not a great T cell depleter. If you give twice the amount of antibody you do not seem to get extra benefit in controling relapses or progression and further supports that stopping cells getting into the CNS stops relapses and stops elements of progression.
As I have said before I think most studies on effects of progression independent of relapse (PIRA) are flawed and a significant element assigned to PIRA is indeed not independent of the effects of relapse. There is data that ocrelizumab and ofatumumab inhibit PIRA and the level of B cell depletion has been associated with the degree of PIRA saying that an important element is by inhibiting B cells in the blood…..Sermon Over:-)
Finally I went to a meeting this week, yep I am not entirely on the maggot pile, and I heard and neuro say that they have only been using early highly effective treatments for well over a year and they said “I don’t recognize PIRA”..This is music to my ears.
Savolainen M, Soilu-Hänninen M, Nurmi H, Viitala M, Tienari P, Atula S, Laakso SM. Comparative Effectiveness and Safety of Rituximab Versus Ocrelizumab in Relapsing-Remitting Multiple Sclerosis: A Finnish Population-Based Matched Cohort Study. Eur J Neurol. 2026 May;33(5):e70625.
Background: B-cell-depleting anti-CD20 therapies are among the most effective disease-modifying treatments for relapsing-remitting multiple sclerosis (RRMS). Rituximab (RTX) is widely used off-label, while ocrelizumab (OCR) is approved for RRMS; yet comparative real-world evidence between the two remains limited.
Methods: We conducted a retrospective registry-based cohort study using the Finnish MS Registry, including adult RRMS patients treated with RTX or OCR between 2018 and 2024 at two university hospitals. Propensity score matching (1:1) was applied to balance baseline characteristics. Primary outcomes were annualized relapse rate (ARR) during follow-up and being relapse-free. Secondary outcomes included MRI activity, disability progression, adverse events, and longitudinal plasma immunoglobulin G (IgG) levels.
Results: Of 636 screened patients, 191 met inclusion criteria and 112 patients (56 RTX, 56 OCR) were included after matching. Median follow-up was 3.1 years for RTX and 2.6 years for OCR. ARR was low and similar in both groups (mean 0.03), and being relapse-free did not differ (log-rank p = 0.95; HR 0.95, 95% CI 0.21-4.33). MRI activity remained largely stable, with no significant differences in T2 lesion changes. Adverse events were infrequent and mild. IgG declined modestly in both groups (mean-13%), with values below the reference range in 4.5% of patients and no association with infections. No disease reactivation was observed among patients switching from OCR to RTX.
Conclusions: In this population-based Finnish real-world study, RTX and OCR demonstrated comparable effectiveness and safety in RRMS, supporting RTX as a rational alternative to OCR in routine clinical practice.
Source: multiple-sclerosis-research.org