I have made the point that the action of anti-CD20 antibodies is probably in the blood and not in the CNS. A trial of double/treble dose of ocrelizumab to help get into the CNS failed to show any extra benefit over the standard dose. In my mind it was always an unlikely result and the idea came from different responses in little and large people but the problem was there was no clear dose-response (Intermediate between Small to Large did not show the expected result) in that data making less likely to be true.
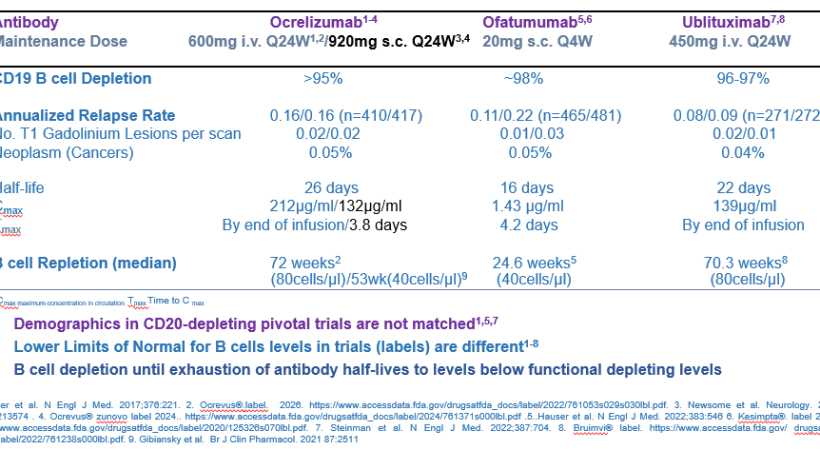
However, the thing I bang on about is the finding that antibodies do not really get into the brain. They are 99.9% excluded from the blood. If this is the case it is unlikely that ofatumumab will be working in the brain. If you look in the label/summary of product characteristics you can see that the maximum concentration of ofatumumab is about 100 times less than other anti-CD20 antibodies. So if antibodies are 99.9% excluded it means the amount entering the brain is about 1ng/ml and that I doubt is enough for a big effect in the CNS and when I am told that this antibody inhibits PIRA, I think PIRA is measuring inhibition of disease in the blood.

We know that antibodies do not get into the CNS very well, because if they did why would you try and develop a new antibody to get into the CNS.

However with rituximab we know what happens to B cells, in the blood, the lymph glands, the spleen, the bone marrow and the brain and yep it is 99.9% excluded. In addition the mechanism of killing by antibodies such as complement mediated killing and antibody-dependent cellular cytotoxicity is less common in the brain than the blood.

In this paper a person treated with rituximab develops a CD20+ B cell cancer in the brain. So the antibody is not getting into the brain to get rid of the cancer.
Harirchian MH, Mohammadianinejad SE, Bayati A, Soleimani V, Sarvestani Z, Kaeedi M, Havadaragh SH. The Sanctuary Within: Development of CD20+ CNS Lymphoma Despite Peripheral B-Cell Depletion by Rituximab in a Multiple Sclerosis Patient. Case Rep Neurol Med. 2026 ;2026:1186165.
Introduction: Patients with multiple sclerosis (MS) are not immune to developing comorbid conditions, including malignant disorders. A new neurologic worsening in a known MS patient, despite being on immunosuppressive or even anti-neoplastic therapy, could be a malignant condition, other than MS relapse.
Case presentation: We report a middle-aged woman with a known history of MS and under treatment with rituximab from a few years ago, who subsequently developed clinical and imaging features that were not typical for MS relapse, which was pathologically confirmed to be a diffuse large B-cell lymphoma (DLBCL).
Conclusion: It is important to consider the possibility of superimposed comorbid disorders, especially malignant conditions, in the setting of immunosuppressive therapy in MS patients. Considering red flags is an important task before the diagnosis of MS relapse as an explanation for new neurologic worsening.
COI: None
Disclaimer: My Views
Source: multiple-sclerosis-research.org