Todays paper triggered my post.
Roostaei T, Fujita M, Touil H, Kivisäkk P, McCabe C, Nejad P, Sabrin A, Garcia FG, van Dorp CH, Felsky D, Vlachos IS, Hui D, Fransson J, Macnair W, Williams A, Zhang L, Zhu W, Xia Z, Zujovic V, Patsopoulos NA, Yates AJ, Kuchroo VK, Chitnis T, Weiner HL, Klein HU, De Jager PL. Cell-type- and state-resolved transcriptomics uncovers distinct T cell and monocyte dysregulation in multiple sclerosis. Cell Rep. 2026 Jun 5;45(6):117417.
Abstract Multiple sclerosis (MS) is a complex immune-mediated disorder with polygenic and multicellular underpinnings, necessitating cell-type-specific molecular studies to delineate dysregulated pathways. Here, we profile 1,075 transcriptomes from 167 patients with MS and 42 healthy participants across six peripheral immune cell-type-states. MS-associated transcriptional differences are more pronounced in primary (unstimulated) immune cells than in in vitro-stimulated counterparts. We identify shared and cell-type-specific transcriptional alterations at the level of genes, pathways, and co-expressed gene modules, prioritizing regulators, such as ZBTB16, across T cells and monocytes, and replicating six MS-associated modules in independent datasets. The top T cell module is enriched for MS susceptibility genes and affects proliferation. The top monocyte module implicates dysregulated TNF-α/NF-κB signaling, for which an in silico drug screen and in vitro validation nominate alvespimycin as a candidate modulator. Together, these findings define stable peripheral immune dysregulation signatures in MS that may serve as diagnostic or prognostic biomarkers in at-risk individuals”.
The post in not about the paper
The academic belief is that MS is a problem of T cells, notably CD4 T cells, and many often ignore the fact that the biology and importantly response to therapy could point elsewhere. Yep I could be wrong, but so far the T cell explanation does not completely compute with the response to therapy. Importantly big pharma largely agree.
Now some B cell inhibitors do not work well enough….BTK inhibitors (B cell inhibitors) for example have not lived up to expectations and some are already on the pharmaceutical maggot pile as far as MS goes.
A next big hope is Frexalimab and some will say “This is a T cell inhibitor”. Yep I say you are correct. I say it blocks CD40 ligand and that is on T cells and not really B cells. It has inhibited relapses. The phase III study will address whether it is better than teriflunomide. Will it be better than anti-CD20?
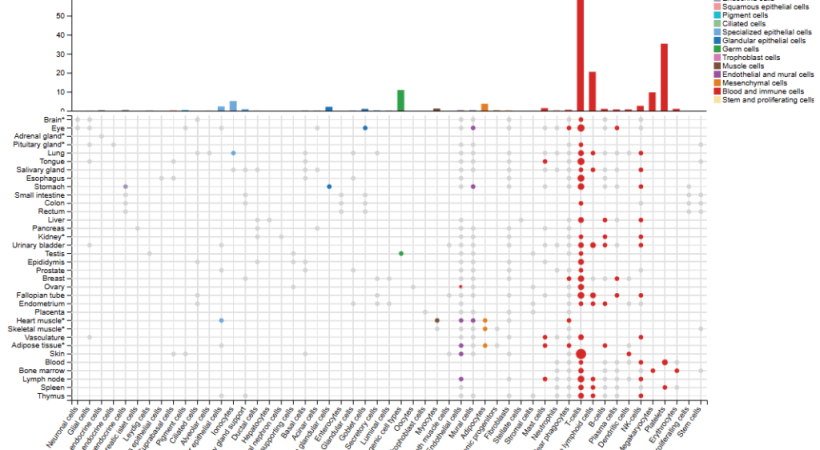
Expression profile of CD40 Ligand. Its on T cells…look at the big red bar below and then the grey bars on the next one down


https://www.proteinatlas.org/ENSG00000102245-CD40LG/single+cell
It’s not on B cells, so is the idea of the importance of B cells wrong?
However this means it will block cells that express CD40 and require CD40 activation to have function and that is….yep you guessed it
B cells
Expression of CD40 on different cell types

And drill down on B cells and yes you guessed it.
Yep memory B cells

https://www.proteinatlas.org/ENSG00000101017-CD40/single+cell
Now that pesky EBV can not only infects B cells and make memory B cells independent of antigenic stimulation because it mimics the signalling of the B cell antigen receptor (The target for the antibodies the B cell will produce). it also makes the CD40 receptor signal that is required with antigen (target) engagement for B cell activation. EBV even makes CD40L and B cell growth factors such as Interleukin-10. The antibody is non depleting. Will it better than teriflunomide. Will it block macrophages?
Early anti-CD40L drugs sometimes caused unwanted platelet aggregation (clumping) leading to blood clots, but frexalimab is specifically engineered with a modified Fc region to prevent this. Will it act on blood vessels in the brain as they can express CD40?. So we have a B cell explanation. Does it deplete memory B cells?…Why look when MS is a T cell problem?.
Todays post only looks at what happens to T cells and monocytes in MS and says they are dyregulated. What happened to B cells?…. Maybe they didn’t look…maybe it is the next paper ,which is better, after they get rid this work…I don’t know…. This study was first reported in BioRXIv in 2022 Cell type- and state- resolved immune transcriptomic profiling identifies glucocorticoid-responsive molecular defects in multiple sclerosis T cells doi: https://doi.org/10.1101/2022.06.29.498195. You can spend a lot of time going down blind alleys and a lot of time publishing. Maybe it leads to Nivana :-(. However, if you focus in the wrong place…your time is wasted. They probably are focussed because they think T cells are all powerful
Indeed this group are champions of the T cells and have been developing anti-CD3 T cell targeting agents, by sniffing them up the nose. So they have T cells top of the agenda, but they are not looking at relapsing MS…but targeting an unmet clinical need….Em.
Non-active progressive MS has not responded well to alemtuzumab, Stem cell therapy, B cell therapy will it respond to T cell therapy when so many other approaches have failed
Anyway if the anti-T cell agent works do you think people will believe that it works because it is targeting B cells?…
Yep CD3 is a classic T cell marker. Likewise CD20 and CD19 are classic B cell markers….But some T cell biologists have convinced themselves that CD20-depleters work because they nibble B cells and take up membrane by a process called trogocytosis. So you have CD20 + and CD3+ T cells. These T cells get depleted by ocrelizumab and hence ocrelizumab works because it depletes T cells.
So I looked for B cell expression and CD3. This occurs very rarely and so there are very, very few CD19+, CD3+ T cells and as CD19+ inhibits lesion formation. like anti-CD20 does also in MS…it means to explain the action of the drug so the mechanism for anti-CD19 and anti-CD20 should be similar. This means one is depleting CD19+, CD20+ B cells as a simple explanation or you have to suggest that they work because they are targetting a very tiny population of T cells. However when you mix B cells and T cells it seems B cells can nibble bits of T cells and they can get CD3 by trogocytosis and so if and when formalumab inhibits relapsing MS…I’ll be waiting I bet there are two chances of that idea making it in print….one is Bob Hope and the other is No Hope:-)
Anyway I digress…as usual. In the paper today they look at gene expression by immune cells and find a signature of T cell proliferation as important. Teriflunomide is a drug designed to inhibit proliferation and B cells proliferate a lot and so are sensitive to anti-proliferation drugs. They find ZBTB16 (Zinc Finger and BTB Domain-Containing 16) which produces a gene production repressor protein that regulates cell cycle progression, stem cell differentiation, and immune system development. However, loss of this gene can also associated with many behavioural issues and cognitive problems and has been associated with impacts on things like develoment of your genitals. Anyway they identify Alvespimycin (also known as 17-DMAG) as a therapeutic and this is an anti-biotic (anti-bacterial drug) that inhibits heat shock protein 90 and is being used as an inhibitor in cancer. However its use in trials were associated with adverse effects leading to termination of development. So not sure where this will go…Scientifically interesting but will it lead to a treatment? Time will tell.
Another compound they pulled out is Ivermectin. This is an interesting drug because it is used in millions of animals and humans to deal with a parasite….However that too leads to another story and that is the fact that ivermectin is actually pumped out of the brain by a molecule called P-glycoprotein that is present on blood vessels of the brain….So that is good news because it is toxic to brain cells and kills some strains of mice and causes problems in Collie dogs that cannot pump the ivermectin out of the brain. I once heard of a story of a cannabis grower who was spraying cannabis plants with ivermectin to kill mites on the crop….They got a neurological problem…Did they express p-glycoprotein or did they lack it?
COI None
Disclaimer My views. Yep much of todays post is not related to the content of the papers mentioned
Source: multiple-sclerosis-research.org